Despite the attention drawn to the topic of concussions over the past decade, it can be difficult to find readily available answers about what parents and young athletes should do after sustaining a concussion.
The Katsuyama family started 2023 without a single concussion, even with quite a few hockey and lacrosse seasons under its belt. That changed when Rylan, 11, received two concussions within five months from sports. One week after Rylan’s second concussion, his brother, Brandon, 13, was illegally checked from behind in a hockey game and sustained his first concussion. After clearing protocol in four weeks, he suffered a second concussion six weeks later.
Both boys endured months of headaches, missed school, dizziness, nausea and the added difficulty of navigating a significant injury peers and adults couldn’t see.
Their father, Brad Katsuyama, co-founder of IEX – a disruptive stock exchange featured in the best-selling book by Michael Lewis, “Flash Boys: A Wall Street Revolt” – sought out expert opinions to guide his family’s decisions and shares some acquired knowledge to help parents and athletes.
1. Brain injuries should be diagnosed by a concussion specialist.
There is no X-ray, MRI or CT scan that can show the extent of most concussion-related injuries, which makes diagnosing them subjective. Symptoms can also appear days after a hit. For example, Brandon was cleared by the emergency room after his first concussion, but two days later failed every test administered by a doctor specializing in concussions.
2.Rushing back to play is one of the worst mistakes you can make.
Experts consistently reinforced that coming back from a concussion too soon can significantly increase long-term brain injury risks. There is likely no tournament, playoff game or tryout worth this risk. An example of how to return smartly is Patrice Bergeron of the National Hockey League’s Boston Bruins, who sat out an entire year to properly heal from a concussion.
“Patrice had four more concussions over his career, and each one was less severe than the last,” renowned concussion specialist Dr. Robert Cantu said. “That wouldn’t have happened without recovery from the first one.”
3.Parents and kids need to be honest about symptoms.
The culture in youth sports praises toughness. Getting your “bell rung” and continuing to play can be viewed as a badge of honor. However, this same mentality can cause athletes to lie to parents, trainers and coaches to get back in the game, which can greatly increase long-term risks. Conversely, the same adults can unduly influence a potentially vulnerable player back on to the field of play. Proper diagnosis requires both adults and athletes to be level-headed and honest in their assessment of concussions.
4. Every person and every concussion is different.
One person’s history and experience with concussions seldom carries any relevance to the concussions experienced by another. For example, Katsuyama played varsity football, hockey and rugby for four years in high school and football in college.
“For the longest time, my definition of a ‘real’ concussion was blacking out, vomiting or pupils dilating,” Katsuyama said. “My sons had none of those symptoms after their hits, but it turns out the severity of their injuries were far greater than anything I had experienced.”
The Katsuyamas turned to the Concussion Legacy Foundation and the Cantu Concussion Center, in addition to their local concussion specialist, to advise their path forward, which has led them to racquet sports and golf in the near-term and long-term playing no more than one contact sport in a school year. Learn more at concussionfoundation.org.
Scientists are probing the head games that influence athletic performance, from coaching to coping with pressure
By Tom Siegfried
Since the early years of this century, it has been commonplace for computerized analyses of athletic statistics to guide a baseball manager’s choice of pinch hitter, a football coach’s decision to punt or pass, or a basketball team’s debate over whether to trade a star player for a draft pick.
But many sports experts who actually watch the games know that the secret to success is not solely in computer databases, but also inside the players’ heads. So perhaps psychologists can offer as much insight into athletic achievement as statistics gurus do.
Sports psychology has, after all, been around a lot longer than computer analytics. Psychological studies of sports appeared as early as the late 19th century. During the 1970s and ’80s, sports psychology became a fertile research field. And within the last decade or so, sports psychology research has exploded, as scientists have explored the nuances of everything from the pursuit of perfection to the harms of abusive coaching.
“Sport pervades cultures, continents, and indeed many facets of daily life,” write Mark Beauchamp, Alan Kingstone and Nikos Ntoumanis, authors of an overview of sports psychology research in the 2023 Annual Review of Psychology.
Their review surveys findings from nearly 150 papers investigating various psychological influences on athletic performance and success. “This body of work sheds light on the diverse ways in which psychological processes contribute to athletic strivings,” the authors write. Such research has the potential not only to enhance athletic performance, they say, but also to provide insights into psychological influences on success in other realms, from education to the military. Psychological knowledge can aid competitive performance under pressure, help evaluate the benefit of pursuing perfection and assess the pluses and minuses of high self-confidence.
Confidence and choking
In sports, high self-confidence (technical term: elevated self-efficacy belief) is generally considered to be a plus. As baseball pitcher Nolan Ryan once said, “You have to have a lot of confidence to be successful in this game.” Many a baseball manager would agree that a batter who lacks confidence against a given pitcher is unlikely to get to first base.
Various studies suggest that self-talk can increase confidence, enhance focus, control emotions and initiate effective actions.
And in fact, a lot of psychological research actually supports that view, suggesting that encouraging self-confidence is a beneficial strategy. Yet while confident athletes do seem to perform better than those afflicted with self-doubt, some studies hint that for a given player, excessive confidence can be detrimental. Artificially inflated confidence, unchecked by honest feedback, may cause players to “fail to allocate sufficient resources based on their overestimated sense of their capabilities,” Beauchamp and colleagues write. In other words, overconfidence may result in underachievement.
Other work shows that high confidence is usually most useful in the most challenging situations (such as attempting a 60-yard field goal), while not helping as much for simpler tasks (like kicking an extra point).
Of course, the ease of kicking either a long field goal or an extra point depends a lot on the stress of the situation. With time running out and the game on the line, a routine play can become an anxiety-inducing trial by fire. Psychological research, Beauchamp and coauthors report, has clearly established that athletes often exhibit “impaired performance under pressure-invoking situations” (technical term: “choking”).
In general, stress impairs not only the guidance of movements but also perceptual ability and decision-making. On the other hand, it’s also true that certain elite athletes perform best under high stress. “There is also insightful evidence that some of the most successful performers actually seek out, and thrive on, anxiety-invoking contexts offered by high-pressure sport,” the authors note. Just ask Michael Jordan or LeBron James.
Many studies have investigated the psychological coping strategies that athletes use to maintain focus and ignore distractions in high-pressure situations. One popular method is a technique known as the “quiet eye.” A basketball player attempting a free throw is typically more likely to make it by maintaining “a longer and steadier gaze” at the basket before shooting, studies have demonstrated.
“In a recent systematic review of interventions designed to alleviate so-called choking, quiet-eye training was identified as being among the most effective approaches,” Beachamp and coauthors write.
Another common stress-coping method is “self-talk,” in which players utter instructional or motivational phrases to themselves in order to boost performance. Saying “I can do it” or “I feel good” can self-motivate a marathon runner, for example. Saying “eye on the ball” might help a baseball batter get a hit.
Researchers have found moderate benefits of self-talk strategies for both novices and experienced athletes, Beauchamp and colleagues report. Various studies suggest that self-talk can increase confidence, enhance focus, control emotions and initiate effective actions.
Moderate performance benefits have also been reported for other techniques for countering stress, such as biofeedback, and possibly meditation and relaxation training.
“It appears that stress regulation interventions represent a promising means of supporting athletes when confronted with performance-related stressors,” Beauchamp and coauthors conclude.
Pursuing athletic perfection
Of course, sports psychology encompasses many other issues besides influencing confidence and coping with pressure. Many athletes set a goal of attaining perfection, for example, but such striving can induce detrimental psychological pressures. One analysis found that athletes pursuing purely personal high standards generally achieved superior performance. But when perfectionism was motivated by fear of criticism from others, performance suffered.
Similarly, while some coaching strategies can aid a player’s performance, several studies have shown that abusive coaching can detract from performance, even for the rest of an athlete’s career.
Beauchamp and his collaborators conclude that a large suite of psychological factors and strategies can aid athletic success. And these factors may well be applicable to other areas of human endeavor where choking can impair performance (say, while performing brain surgery or flying a fighter jet).
But the authors also point out that researchers shouldn’t neglect the need to consider that in sports, performance is also affected by the adversarial nature of competition. A pitcher’s psychological strategies that are effective against most hitters might not fare so well against Shohei Ohtani, for instance.
Besides that, sports psychology studies (much like computer-based analytics) rely on statistics. As Adolphe Quetelet, a pioneer of social statistics, emphasized in the 19th century, statistics do not define any individual — average life expectancy cannot tell you when any given person will die. On the other hand, he noted, no single exceptional case invalidates the general conclusions from sound statistical analysis.
Sports are, in fact, all about the quest of the individual (or a team) to defeat the opposition. Success often requires defying the odds — which is why gambling on athletic events is such a big business. Sports consist of contests between the averages and the exceptions, and neither computer analytics nor psychological science can tell you in advance who is going to win. That’s why they play the games.
People with outward appearances of success, productivity and happiness often still deal with internal struggles. Mental health challenges continue to affect Americans, with nearly 3 of 4 (73%) U.S. adults reporting struggles with mental health in 2023.
These findings come from a mental health survey commissioned by RedBox Rx, a telehealth and online pharmacy provider, and conducted by Morning Consult.
“Mental health remains a struggle for many Americans,” said Dr. Daniel Fick, RedBox Rx’s chief medical officer. “The findings from this study demonstrate more resources and support are needed to help individuals manage their mental health, especially younger adults. We are focused on fulfilling this need by offering easy-to-access, affordable, discreet and convenient telehealth care and treatment for those struggling with mental health.”
In honor of Mental Health Awareness Month, consider these mental health trends identified in the survey:
1. Younger Generations are More Likely to Report Mental Health Struggles, Worsening Mental Health
Gen Zers and Millennials are more likely to report having mental health struggles and more likely to say those struggles worsened in the past year. In fact, 41% of Gen Zers and 36% of Millennials reported more mental health struggles in the past year compared with 21% of adults ages 45 and older.
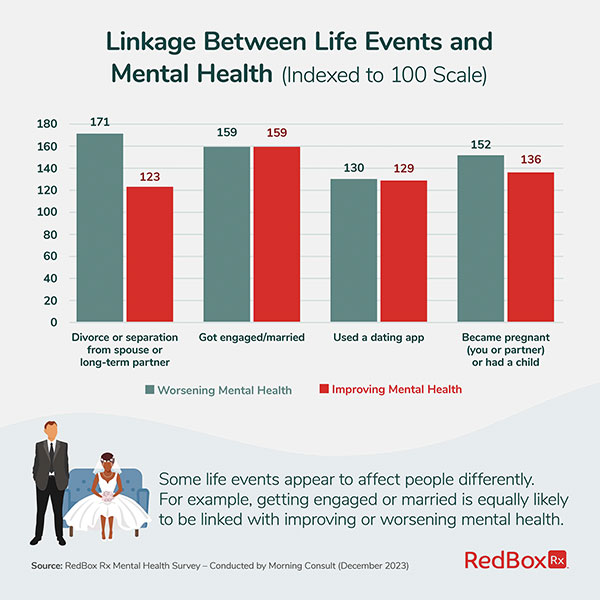
2. Specific Life Events Affect People Differently
Some life events appear to affect people differently. For example, getting divorced or separated and becoming pregnant or having a child are linked with both worsening and improving mental health. Getting engaged or married and using a dating app are equally likely to be linked with both positive and negative impacts on mental health.
3. Younger Generations Endure Life Events Linked with Worsening Mental Health
Gen Zers and Millennials more frequently experience life events having the strongest links to worsening mental health. They more commonly report loneliness and a failure to achieve life goals, stressors also linked to worsening mental health. For example, 53% of Gen Zers reported feelings of loneliness and 52% shared feelings of failure to achieve life goals, compared with 39% and 34%, respectively, of all adults sampled.
The research also found recent life experiences, whether relational or personal, are linked to the state of one’s mental health. Those suffering from worsening mental health were more likely to have experienced:
Being a victim of verbal or emotional abuse
Being a victim of physical violence
The lack of a healthy home environment
The lack of a healthy work environment
Attending college or university
The breakdown in a relationship with a close family member
According to the study, if you’ve experienced verbal or emotional abuse – which is 12% more prevalent among Gen Zers – you are more than twice as likely to report worsening mental health.
4. Despite Mental Health Struggles, Most Americans Aren’t Seeking Professional Care
Even though mental health struggles are widespread among American adults, more than 6 out of 10 (63%) with consistent or worsening mental health struggles have not sought professional care, such as therapy or medications, in the past year.
Those not seeking care tend to downplay their situations or cite the cost of care as a barrier. Through its discreet, low-cost service model, RedBox Rx’s online platform makes it easy for patients to quickly schedule telehealth visits and privately meet with licensed medical providers to get help with treating a variety of mental health conditions including anxiety and depression, adult ADHD and insomnia.
“Telehealth offers an effective and convenient way for patients to easily access care for mental health conditions,” Fick said.
To view the full report, access infographics from the study and find more information about mental health therapy and medical treatments, visit RedBoxRx.com.
New research suggests that to maintain a healthy brain, we should tend our gut microbiome. The best way to do that right now is not through pills and supplements, but better food.
By Tim Vernimmen -Neuroscientist John Cryan Q&A
It is increasingly well understood that the countless microbes in our guts help us to digest our food, to absorb and produce essential nutrients, and to prevent harmful organisms from settling in. Less intuitive — perhaps even outlandish — is the idea that those microbes may also affect our mood, our mental health and how we perform on cognitive tests. But there is mounting evidence that they do.
For nearly two decades, neuroscientist John Cryan of University College Cork in Ireland has been uncovering ways in which intestinal microbes affect the brain and behavior of humans and other animals. To his surprise, many of the effects he’s seen in rodents appear to be mirrored in our own species. Most remarkably, research by Cryan and others has shown that transplanting microbes from the guts of people with psychiatric disorders like depression to the guts of rodents can cause comparable symptoms in the animals.
These effects may occur in several ways — through the vagus nerve connecting the gut to the brain, through the influence of gut bacteria on our immune systems, or by microbes synthesizing molecules that our nerve cells use to communicate. Cryan and coauthors summarize the science in a set of articles including “Man and the Microbiome: A New Theory of Everything?,” published in the Annual Review of Clinical Psychology. Cryan told Knowable Magazine that even though it will take much more research to pin down the mechanisms and figure out how to apply the insights, there are some things we can do already.
This conversation has been edited for length and clarity.
“Man and the Microbiome: A New Theory of Everything?” — with all due respect, isn’t that a wee bit ambitious?
That title is admittedly a bit overstated. But the point we are trying to make is that it isn’t really so odd that the microbiome is involved in everything, because the microbes were there first, and so our species has evolved in their presence. We have been able to show that growing up in a germ-free environment really affects the development of the mouse brain, for example, in a variety of ways.
Our immune system is also completely shaped by microbial signals. Via that route, inflammation in our gut can affect our mood and cause symptoms of sickness behavior that are quite similar to important aspects of depression and anxiety. Many psychiatric disorders are also known to be associated with various gastrointestinal issues, though cause and effect often aren’t clear yet. So if you study the body, including the brain, you ignore microbes at your own peril.
Most people are on board with the idea that gut microbes affect our health, but it may be more difficult to accept that they also influence how we feel and think. How did you convince yourself this was true?
I’m a stress neurobiologist, so I was trained in stress-related disorders like depression and anxiety, and my interest was really in using animal models of stress to look for novel therapeutic strategies.
When I moved to University College Cork in 2005, I met a clinical researcher, Ted Dinan, and we started working together to study irritable bowel syndrome, a very common disorder that is characterized by alterations in bowel habits and abdominal pain.
That was interesting to me, as it had become very clear that this is also a stress-related disorder. So we started working on an animal model called the maternal separation model, where rat pups are separated from their moms early in life and develop a stress-like syndrome when they grow up.
Siobhain O’Mahony, a graduate student at the time, also wanted to look at the microbiome, and I remember telling her, “No! Focus, focus!” But she went ahead anyway and found a signature of this early-life stress in the microbiome of adult rats. That was kind of a eureka moment for me.
The next part of the puzzle came when we showed that mice born in a germ-free environment have an exaggerated stress response when they grow up. So we’d already shown that stress was affecting the microbiome, and now we’d shown that the microbiome is regulating how a mouse responds to stress. It turned out that a very nice study from Japan had already shown this.
The third part of the puzzle for me was to ask whether we could alter the microbiome to alleviate some of the effects of stress. In 2011, we were able to show that a specific strain of the bacterium Lactobacillus, when given to normal, healthy mice in a stressful situation, was able to dampen down the stress response, and that the vagus nerve connecting the gut to the brain was required for that.
These three things together, from 2006 to 2011, really crystallized my interest in the link between the gut microbiome, brain and behavior. Since then, we’ve been on this magical journey to try and understand these discoveries, uncover the mechanisms and find how they translate to humans.
Can you explain what a depressed or anxious mouse looks like, and how you quantify that?
One way to look at fear is to quantify how often mice venture into wide open areas, which they normally avoid. If we give a mouse Valium or another anxiety-reducing drug, it will go out and explore and be carefree, not to say a bit reckless. Depression is often studied by looking at mice in a cylinder of water. They are good swimmers, but they don’t like swimming, so after a while, they’ll stop and adopt an immobile posture. Yet if you give them antidepressant drugs, they keep going.
These types of paradigms have shown their validity in studies of pharmacological agents used in human psychiatry, and so they’re ideal to explore whether microbiome manipulations have similar effects. This can be done by transplanting the microbes from a mouse model for a psychiatric disease to a healthy mouse to see whether that creates similar issues, or vice versa, to see if it can resolve them.
Following a similar logic, we have shown that the microbiome can be important in brain aging and cognitive decline. We took the microbiome from eight-week-old mice and gave it to 22-month-old animals — these are very old mice. And we were able to show wide-scale changes across the body — in the microbiome and the immune system, but also in the hippocampus, a brain structure involved in memory.
In the old animals that received the microbiome from young ones, the hippocampus looked completely rejuvenated in its chemical composition. They also performed significantly better in mazes designed to test their memory. This finding has now been replicated in two other labs, giving it further credence.
Such experiments are difficult if not impossible to do in people. How to make that jump?
One thing we can do is to transplant microbes from the guts of people with psychiatric disorders to rodents, to see if they cause comparable behaviors. This has now been done for depression, anxiety, schizophrenia, social anxiety disorder and even Alzheimer’s disease. In one of our own studies, we transferred fecal microbiota from depressed patients to a rat model. This resulted in behavior reminiscent of that in rat models for depression, such as increased anxiety and an uninterest in rewards, in addition to inflammation.
In addition, we can see if bacterial strains we’ve identified as troublemakers in rodents also occur in people with psychiatric issues, and if strains that are beneficial in rodents can help humans as well.
What I’d really like to do is follow a large group of healthy people for a couple of years and track their mental and brain health as well as the changes in their microbiome, and regularly transplant their gut microbes into mice. This would give us a much better view on how this relationship evolves.
Do you think some of the probiotics available in stores today might be helpful, or not quite?
In my opinion, many so-called probiotics aren’t probiotics at all. Probiotics, per definition, are live microorganisms that, when taken in adequate amounts, can confer a health benefit. Most of what’s for sale in shops would never meet that criterion. To demonstrate that something confers a health benefit, you need clinical trials to show it is more effective than a placebo. That’s the first thing. Second, you have to show that the microbes are alive, and that they can survive the stomach acid.
There have been properly randomized controlled trials for some products. But for most products available over the counter today, such studies haven’t been done, because the regulatory authorities do not require them for probiotics as they would for medicines.
There’s a lot of snake oil out there. For most people, it’s probably harmless, but if you are immunosuppressed, it could be dangerous: Even beneficial bacteria can cause great harm if your immune system does not function properly.
Don’t get me wrong, I think there are many promising findings, but this field is very much in its infancy. I’m much more enthusiastic right now about whole-food approaches that adjust people’s diets to include more fermented foods — a source of beneficial bacteria — and the fibers that many beneficial members of our microbiome need to survive. And this, everyone can already do.
Have you done any experiments that show such a diet can improve mental health?
We’ve just done a small study with what we call a psychobiotic diet. Kirsten Berding, a German dietician who did a post-doc in my group, took a group of people with bad diets who were stress-sensitive — namely, our student population — and put them on a one-month diet to really ramp up fermented foods and fibers to the benefit of the microbiome. What we showed was that the better individuals followed the diet, the greater the reduction in stress.
The study wasn’t perfectly blinded, because people knew what they were eating, but they didn’t know what they were eating it for. And this was just the beginning: We’re now doing a much longer study trying to really untangle this.
We’ve also done a small randomly controlled study with a polydextrose fiber that was shown to improve the performance of healthy volunteers on a range of cognitive tests.
Obviously, more work of this kind is necessary. But in this case, I don’t think we should wait for that. Think about the experiment where we’ve transplanted microbes from young to old mice, for example: I’m not advertising poop transplants for aging adults. What we’ve found is that the more diverse your diet, the more diverse your microbiome, and the better your health when you get old. If you look at the beige, bland food served in many nursing homes and hospitals today, that is not the kind of diet that helps people to maintain a healthy microbiome and therefore a healthy brain.
“Perhaps if you’re thinking of having a midlife crisis, forget about the motorbike and start growing vegetables.”
— JOHN CRYAN
We’ve done a study in mice where we adjusted their diet to contain much more inulin, a fiber that we know supports the growth of beneficial bacterial strains, and found we could dampen down the neuroinflammation that is often associated with cognitive decline in aging. This fiber is present in our everyday diet — there is a lot of it in vegetables like leeks, artichokes and chicory. So perhaps if you’re thinking of having a midlife crisis, forget about the motorbike and start growing vegetables.
This is all in healthy patients. Do you think the diet might also help people with mental health issues?
I do, but we need to test it, of course.An earlier study of ours showed that students born by C-section, who missed out on some of the microbes that newborns acquire during vaginal birth, had an elevated immune and psychological response to both chronic and acute stress, in line with our findings in mice. It would be very interesting to test if a psychobiotic diet might benefit them.
As I said, many psychiatric disorders are also associated with inflammation and other problems in the gut. Of course, this relationship works both ways, and it’s not always clear to what extent the irregularities in the gut are the cause or the result of the mental issues — or whether it’s a bit of both. But if we can show a healthier microbiome can improve mental health, that would be great news.
This is what’s appealing about the microbiome: It’s probably more modifiable than the rest of our body. If we understand how it works, that might give people more options to improve their health, even if they didn’t have the best start, microbially speaking. That’s what we hope to achieve.
The research looked at the results of 31 studies and a total sample of more than 60,000 students.
monkeybusinessimages/iStock via Getty Images PlusChristina Scherrer, Kennesaw State University and Shillpa Naavaal, Virginia Commonwealth University
Programs delivering fluoride varnish in schools significantly reduce cavities in children. That is a key finding of our recently published study in the American Journal of Preventive Medicine.
Fluoride varnish is a liquid that is applied to the teeth by a trained provider to reduce cavities. It does not require special dental devices and can be applied quickly in various settings.
Our research team found that school fluoride varnish programs, implemented primarily in communities with lower incomes and high cavity risk among children, achieve meaningful rates of student participation and reduced new cavities by 32% in permanent teeth and by 25% in primary – or “baby” – teeth.
We also found that school fluoride varnish programs reduced the progression of small cavities to more severe cavities by 10%. This positive impact held true among school children of various ages in preschool through high school, in rural or urban areas and in communities with and without fluoridated tap water. Fluoride varnish remained effective when delivered by various providers, including dentists, hygienists or trained lay workers.
This research was a large team collaboration on a systematic review, led by researchers from the Centers for Disease Control and Prevention and from our universities. A systematic review is when researchers carefully collect and study all the best available research on a specific topic to figure out what the overall evidence shows.
Ultimately, our conclusions were based on 31 published studies that were reported in 43 peer-reviewed articles involving 60,780 students.
In addition, we believe that since there is a growing movement in the U.S. to remove water fluoridation, other ways of protecting teeth with fluoride, such as toothpaste and varnish, will become more important. About three-quarters of the U.S. population using public water systems has been receiving fluoridated water at levels designed to strengthen enamel and prevent cavities. They will be at higher risk for cavities if fluoride is removed from their drinking water.
This makes schools an important setting for delivery of fluoride varnish to increase access. Students typically receive a dental exam, oral health education and supplies, and referrals for dental care. Depending on state regulations, the varnish can be applied by dental and medical professionals or trained lay workers.
Limited funds are a barrier. We believe that further understanding the ways to reduce the cost of these programs would help to expand them and reach more students.
One key opportunity is relaxing the restrictions on application by health professionals such as medical assistants and registered nurses, which is allowed in some states but not others.
Programs also sometimes struggle to get schools and families fully engaged. More research could help us determine the best ways to increase the percentage of families that return their consent forms and make school fluoride programs easier to run.
Another barrier is that many states only provide insurance reimbursement for these programs through age 6. Thus, increasing the eligibility age served by medical providers can serve more children, increase the number of these programs and protect more children’s teeth from decay – supporting oral and overall health.
The Research Brief is a short take on interesting academic work.
Christina Scherrer, Professor of Industrial and Systems Engineering, Kennesaw State University and Shillpa Naavaal, Associate Professor of Pediatric Dentistry, Virginia Commonwealth University
This article is republished from The Conversation under a Creative Commons license.
Strokes can happen to anyone, at any age – even young people. Despite being one of the leading causes of death and long-term disability in the United States, strokes are largely preventable, treatable and beatable – if you can control your risk factors.
According to the American Stroke Association, a division of the American Heart Association, every 40 seconds, someone in the U.S. has a stroke. Keeping blood pressure in check, living a healthy lifestyle and knowing stroke warning signs may help protect you and your loved ones.
Here are key insights from the American Stroke Association’s Together to End Stroke initiative, nationally supported by the HCA Healthcare Foundation.
Controlling Risk Factors
Up to 80% of strokes may be preventable, according to the American Stroke Association. You can take action to prevent strokes by managing your risk factors, like high blood pressure, a leading cause and controllable risk factor for stroke and heart disease.
Other risk factors include diabetes and obesity, which can be kept in check with healthy lifestyle behaviors such as good nutrition. Quitting smoking and being physically active are important. Atrial fibrillation, or AFib, which is a quivering or irregular heartbeat, also increases stroke risk. In fact, people with AFib are five times more likely to have a stroke, according to the American Heart Association.
Preventing a Second Stroke
Nearly 1 in 4 strokes occur in people who had a previous stroke, sometimes because they don’t know what caused the first, making identifying the cause of the stroke a key step toward future prevention. Treatment depends on the type of stroke someone is having, which can be determined with a series of medical evaluations and tests.
Work with your health care professional to develop a plan that helps you move forward after a first stroke while preventing a second. This plan should include controlling risk factors, like achieving and maintaining healthy blood pressure, blood sugar and cholesterol levels.
“Preventing a second stroke is possible with the right approach,” said Teresita Casanova, MD, HCA Healthcare affiliated neurologist and American Stroke Association volunteer expert. “Taking medicines as prescribed, monitoring health numbers, and making small, consistent lifestyle changes can make a big difference. Stroke survivors should feel empowered to take control of their health and work with their care team to build a strong prevention plan.”
To help you in your journey, you can rely on tools such as the Heart & Stroke Helper, a free self-management app available for stroke survivors and their caregivers. The app allows patients to oversee their health in one place with features that track progress on lifestyle habits, manage medications, track health numbers, provide information about stroke and allow patients to connect with others for inspiration.
Find more ways to manage second stroke risk at Stroke.org
Act F.A.S.T.: How to Detect Signs of Stroke
Most adults in the U.S. don’t know the stroke warning signs, nor that stroke is largely treatable if you call 911 as soon as you recognize the symptoms.
Learning the acronym F.A.S.T. can help you recognize that someone may be having stroke symptoms so you can take life-saving action.
F: Face Drooping. Does one side of the face droop, or is it numb? Ask the person to smile. Is the person’s smile uneven?
A: Arm Weakness. Is one arm weak or numb? Ask the person to raise both arms. Does one arm drift downward?
S: Speech. Is speech slurred? Is the person unable to speak or hard to understand? Ask the person to repeat a simple sentence, like “The sky is blue.”
T: Time to Call 911. If you or anyone else shows any of these symptoms, call 911 immediately.
It’s no secret that many grocery store dairy sections are filled with more options today. One choice continuing to gain favor with consumers is 100% grass-fed organic dairy. Nutrition, environmental awareness and animal care are some of the leading reasons consumers choose grass-fed dairy products.
Globally, the 100% grass-fed dairy market is projected to continue growing and some market experts predict annual growth rates as high as 22%. If you’re curious about 100% grass-fed organic dairy, consider these benefits from Maple Hill, America’s original 100% grass-fed organic dairy producer. The pioneer of 100% grass-fed organic dairy took its commitment a step further by celebrating and declaring National 100% Grass-Fed Organic Dairy Day on April 15, which recognizes the positive impact it has on consumers, cows, farmers and the environment.
1. Honoring the Farmers
Unlike large-scale corporate dairy farms, most organic farms are small, family-owned operations dedicated to traditional, sustainable farming. Small dairy farms have been disappearing, but 100% grass-fed organic dairy creates a sustainable, viable path forward for farmers who work in harmony with nature.
This more natural approach to dairy is a “craft” process favoring small family farmers who are willing to dedicate the extra focus and patience to a better product and process. These family farms are passed on to future generations to grow the “better for you, better for the planet” approach.
2. Commitment to Good Health
Most consumers don’t know the difference between traditional organic and 100% grass-fed organic dairy. One key distinction is the products’ nutritional composition; 100% grass-fed organic dairy provides a 50% healthier ratio of omega 3:6 and 40% higher levels of CLA fatty acids, which may support heart health and provide other health benefits.
What’s more, Maple Hill’s products made with 100% grass-fed organic dairy are GMO free, hormone free and antibiotic free with no additives or fillers. The line of high-quality, rich-flavored products let you experience the organic difference from traditional dairy for a nutrient-dense solution that tastes as nature intended.
3. Happy, Healthy Cows
Cows on a 100% grass-fed diet can live up to three times as long as grain-fed cows and are never subjected to unnatural diets, hormones or antibiotics. More time in pastures filled with lush grass means cows have the freedom to roam, ruminate and graze on diverse, nutrient-rich grasses.
The result is happier, healthier cows, which in turn results in a richer, better-tasting and more nutrient-dense milk.
4. Sustainability and the Environment
Producing milk without grain or corn requires farmers to focus on regenerating soil and the soil life that supports everything else on the farm. In fact, the healthier the soil, the healthier the feed, so farmers have a natural incentive to be as regenerative as possible. Regenerative grazing practices are a powerful and positive tool to improve land and the web of life on farms by actively restoring soil health, promoting biodiversity and reducing the environmental impact compared to conventional dairy.
Well-managed grazing helps pull carbon from the atmosphere into the soil, fighting climate change in the process. In addition, healthier soil retains more water, reducing runoff and protecting water sources from agricultural pollution.
5. Strengthening the 100% Grass-Fed Organic Market
Consumers are increasingly aware of the choices they have in dairy products and how 100% grass-fed organic supports their health, farmers, animals and the planet. Some ways to support this category’s continued growth include choosing certified 100% grass-fed organic dairy, advocating for regenerative farming and helping shape a more sustainable food system.
Learn more about 100% grass-fed organic dairy products at maplehill.com.
More than 4.2 million Americans live with glaucoma, a leading cause of vision loss in the nation. Although there is no cure for glaucoma, early detection and treatment can stop this condition in its tracks.
“Glaucoma is a leading cause of vision loss and blindness in the United States, but it’s estimated that half of people with glaucoma don’t know they have it,” said Michael F. Chiang, M.D. “Glaucoma has no early symptoms, and the only way to check if you have it is to get a comprehensive dilated eye exam. There’s no cure for glaucoma, but starting treatment as early as possible can help stop vision loss.”
Regular eye exams are among the best lines of defense because symptoms may not appear until the disease has progressed significantly. Knowing more about how to spot the condition and what you can do about it may help protect your vision in the long run.
Glaucoma is actually a group of eye diseases that damage the optic nerve in the back of the eye and cause vision loss and blindness. The most common type in the United States is open-angle glaucoma. Other, less common, types include angle-closure glaucoma and congenital glaucoma.
Learn more about glaucoma from the experts at the National Eye Institute in honor of Glaucoma Awareness Month.
Causes
For some people, glaucoma is the result of another medical condition, but that’s not always the case. While experts still aren’t sure exactly what causes open-angle glaucoma, it’s believed to be related to the pressure that builds in the eye when fluid doesn’t drain fast enough. Over time, the pressure causes nerve damage, which then leads to vision loss.
Risk Factors
Glaucoma is not preventable and can affect anyone. However, some groups of people are at higher risk, including those over age 60 – particularly Hispanic or Latino individuals. African American individuals over age 40 are also at greater risk, as are people with a family history of glaucoma.
Symptoms
Early on, most people do not experience any symptoms of glaucoma. Over time, you may start to notice disruptions to your vision, such as blind spots or decreased peripheral vision (what you see from the sides of your eyes) in one or both eyes. This loss may be especially prevalent closest to your nose. Symptoms typically progress so slowly that people get used to it and don’t realize their vision is changing, which is why so many people with glaucoma don’t know they have it.
Intense eye pain, nausea, red eyes and blurry vision are all potential signs of angle-closure glaucoma, and immediate emergency treatment is necessary.
Diagnosis
The only way to properly diagnose glaucoma is through a dilated eye exam, including visual field testing to check your side vision. This routine test is painless and involves looking straight ahead while your doctor checks how well you can see objects off to the side or at the top or bottom of your field of vision.
Treatment
Without treatment, glaucoma can eventually lead to blindness. Treatment won’t undo any vision damage, but it can stop it from getting worse. Treatment may involve prescription eye drops to reduce eye pressure. Other treatment options include a laser procedure or surgery to help fluid drain. Vision rehabilitation services and devices may help if vision loss affects your everyday activities.
Dr. Julio Fernandez-Mendoza is a professor of psychiatry and behavioral health, neuroscience and public health sciences at Penn State College of Medicine. He discusses the need for sleep, why teenagers require more sleep than adults, and how you can get a good night’s sleep without medications.
Julio Fernandez-Mendoza discusses heart health and sleep.
The Conversation has collaborated with SciLine to bring you highlights from the discussion that have been edited for brevity and clarity.
How much sleep is enough for adults and for adolescents?
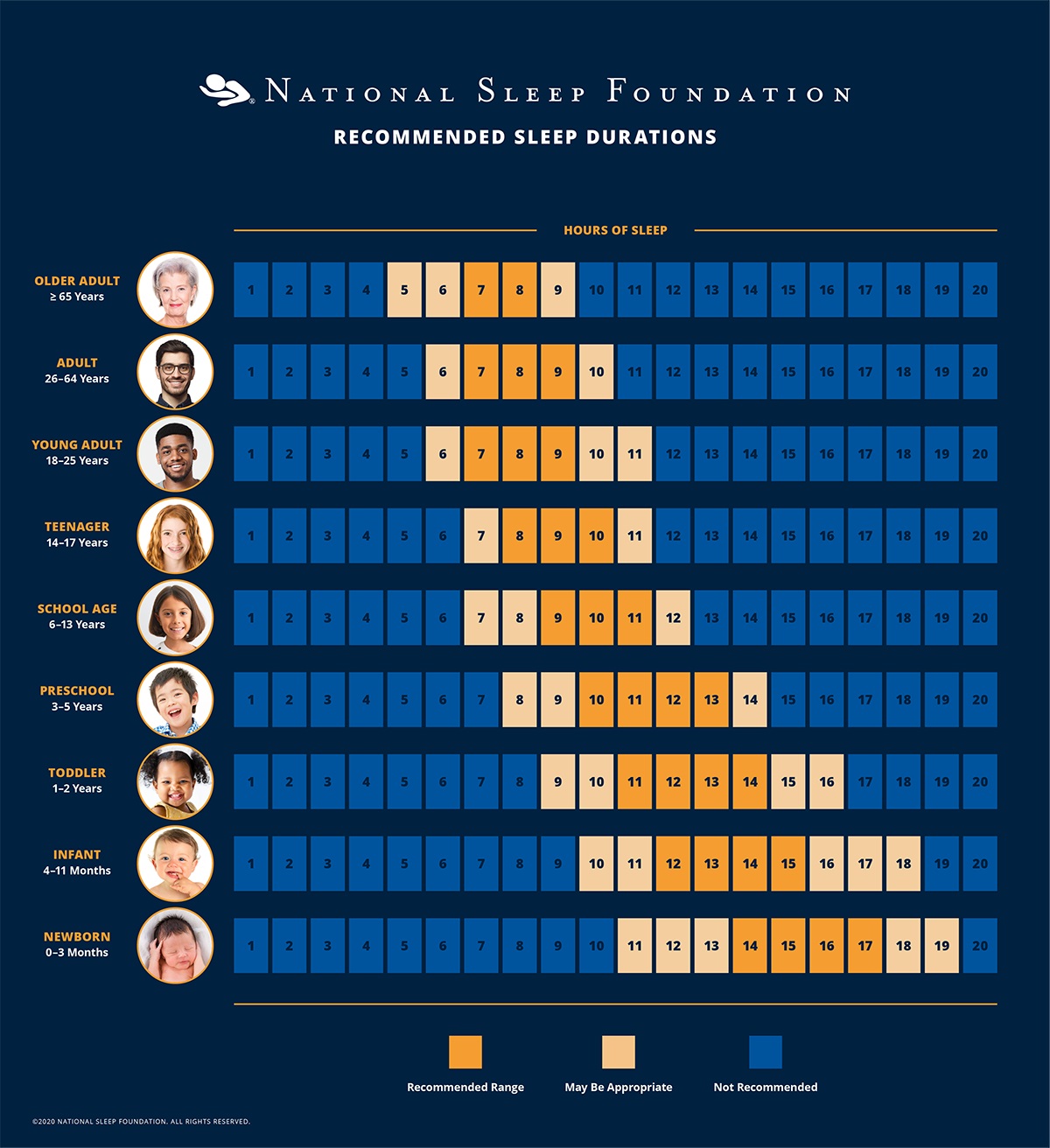
Julio Fernandez-Mendoza: Adults who report getting about seven to eight hours of sleep per night generally have the best health, in terms of both physical and mental health, and longevity.
But that recommendation changes with age. Adults over age 65 may need just six to seven hours of sleep per night. So older people, if otherwise healthy, should not feel anxious if they’re getting just six hours. Young people need the most – at least nine hours – and some younger children may need more.
How can insufficient sleep harm our health?
Fernandez-Mendoza: Our team was the first to show that those complaining about insomnia – difficulty falling or staying asleep – were more likely to have high blood pressure and be at risk for heart disease.
What about people who have more serious sleep problems?
Fernandez-Mendoza:Good sleep hygiene habits include cutting down on caffeine and alcohol, quitting smoking and exercising regularly. I also recommend not skipping meals, not eating too late at night and not eating too much.
But people with a persistent sleep problem may need to make more behavioral changes. Research studies point to a set of six rules that can improve your sleep. You can follow these changes consistently in the short term, and then choose how to adapt them into your lifestyle down the road.
First, get up at the same time no matter what. No matter how much sleep you get. This will anchor your sleep/wake cycle, called your circadian rhythm.
Second, do not use your bed for anything except sleep and sexual activity.
Third, when you can’t sleep, don’t lie in bed awake. Instead, get out of bed, go into another room if you can, and do an activity that’s enjoyable or relaxing. Go back to bed only when you’re ready to sleep.
Fourth, get going with daily activities even after a poor night’s sleep. Don’t try to compensate for sleep loss. If you have chronic insomnia, don’t nap, sleep in, or doze during the day or evening even after poor sleep the previous night.
Fifth, go to bed only when you’re actually sleepy enough to fall asleep.
And sixth, start with the amount of sleep you’re now getting – with the lowest limit at five hours – and then increase it weekly by 15 minutes.
These six rules are evidence-based and go above and beyond simple sleep hygiene habits. If they don’t work, see a provider who can help you.
Your teen isn’t lazy. There are reasons why adolescents sleep in.
Do you have advice specifically for adolescents?
Fernandez-Mendoza: Adolescence is a unique developmental period. It’s not just the obvious physical, emotional and behavioral changes that occur during adolescence and puberty – there are changes in a teenager’s brain that can alter their sleep patterns.
When an adolescent goes through puberty, their internal clock changes so that their sleep schedule shifts to later hours. While it’s true that adolescents are more engaged at night because of their social relationships, there’s also biology behind why they want to stay up late – their internal clocks have shifted. It’s not just choice.
Parents can help their teens get better sleep. Set a time for kids to stop doing homework and put away electronics. Instead, they can watch TV with the family or read – something relaxing and enjoyable that will help them wind down before bed.
You can also gradually move back their wake-up time. Start on weekends, waking them up 30 minutes earlier every day, including school days, until the child reaches the desired wake-up time. Don’t try to reshift them suddenly – for example, waking up a teenager at 5 a.m. like it’s the military – because that doesn’t work. They won’t get used to it, since it’s at odds with their internal clock. So, do it little by little. If that doesn’t work, see a clinical provider.
What kind of treatments can a sleep clinician provide?
Fernandez-Mendoza: People should get help if they feel they sleep poorly, if they’re fatigued during the day, or if they snore or grind their teeth. All these issues deserve attention.
Some people may think a sleep provider just prescribes expensive medication, but that’s not true. There are behavioral, non-drug-based treatments that work. Cognitive behavioral therapy is the first-line treatment recommended for insomnia. Light therapy may also help, which is the use of a bright light therapy lamp at a given time during the day or evening, depending on the person’s sleep problem.
SciLine is a free service based at the American Association for the Advancement of Science, a nonprofit that helps journalists include scientific evidence and experts in their news stories.
Julio Fernandez-Mendoza, Professor of Psychiatry and Behavioral Health, Neuroscience, and Public Health Sciences, Penn State
This article is republished from The Conversation under a Creative Commons license.
It can take a lot of effort to understand the many different Medicare choices.
Halfpoint Images/Moment via Getty ImagesGrace McCormack, University of Southern California and Melissa Garrido, Boston University
The 67 million Americans eligible for Medicare make an important decision every October: Should they make changes in their Medicare health insurance plans for the next calendar year?
The decision is complicated. Medicare has an enormous variety of coverage options, with large and varying implications for people’s health and finances, both as beneficiaries and taxpayers. And the decision is consequential – some choices lock beneficiaries out of traditional Medicare.
Beneficiaries choose an insurance plan when they turn 65 or become eligible based on qualifying chronic conditions or disabilities. After the initial sign-up, most beneficiaries can make changes only during the open enrollment period each fall.
The 2024 open enrollment period, which runs from Oct. 15 to Dec. 7, marks an opportunity to reassess options. Given the complicated nature of Medicare and the scarcity of unbiased advisers, however, finding reliable information and understanding the options available can be challenging.
We are health carepolicy experts who study Medicare, and even we find it complicated. One of us recently helped a relative enroll in Medicare for the first time. She’s healthy, has access to health insurance through her employer and doesn’t regularly take prescription drugs. Even in this straightforward scenario, the number of choices were overwhelming.
The stakes of these choices are even higher for people managing multiple chronic conditions. There is help available for beneficiaries, but we have found that there is considerable room for improvement – especially in making help available for everyone who needs it.
The choice is complex, especially when you are signing up for the first time and if you are eligible for both Medicare and Medicaid. Insurers often engage in aggressive and sometimes deceptive advertising and outreach through brokers and agents. Choose unbiased resources to guide you through the process, like www.shiphelp.org. Make sure to start before your 65th birthday for initial sign-up, look out for yearly plan changes, and start well before the Dec. 7 deadline for any plan changes.
2 paths with many decisions
Within Medicare, beneficiaries have a choice between two very different programs. They can enroll in either traditional Medicare, which is administered by the government, or one of the Medicare Advantage plans offered by private insurance companies.
Within each program are dozens of further choices.
Traditional Medicare is a nationally uniform cost-sharing plan for medical services that allows people to choose their providers for most types of medical care, usually without prior authorization. Deductibles for 2024 are US$1,632 for hospital costs and $240 for outpatient and medical costs. Patients also have to chip in starting on Day 61 for a hospital stay and Day 21 for a skilled nursing facility stay. This percentage is known as coinsurance. After the yearly deductible, Medicare pays 80% of outpatient and medical costs, leaving the person with a 20% copayment. Traditional Medicare’s basic plan, known as Part A and Part B, also has no out-of-pocket maximum.
People enrolled in traditional Medicare can also purchase supplemental coverage from a private insurance company, known as Part D, for drugs. And they can purchase supplemental coverage, known as Medigap, to lower or eliminate their deductibles, coinsurance and copayments, cap costs for Parts A and B, and add an emergency foreign travel benefit.
The Medicare Advantage program allows private insurers to bundle everything together and offers many enrollment options. Compared with traditional Medicare, Medicare Advantage plans typically offer lower out-of-pocket costs. They often bundle supplemental coverage for hearing, vision and dental, which is not part of traditional Medicare.
Understanding the tradeoffs between premiums, health care access and out-of-pocket health care costs can be overwhelming.
Turning 65 begins the process of taking one of two major paths, which each have a thicket of health care choices.Rika Kanaoka/USC Schaeffer Center for Health Policy & Economics
Different Medicare Advantage plans have varying and large impacts on enrollee health, including dramatic differences in mortality rates. Researchers found a 16% difference per year between the best and worst Medicare Advantage plans, meaning that for every 100 people in the worst plans who die within a year, they would expect only 84 people to die within that year if all had been enrolled in the best plans instead. They also found plans that cost more had lower mortality rates, but plans that had higher federal quality ratings – known as “star ratings” – did not necessarily have lower mortality rates.
While many Medicare Advantage plans boast about their supplemental benefits , such as vision and dental coverage, it’s often difficult to understand how generous this supplemental coverage is. For instance, while most Medicare Advantage plans offer supplemental dental benefits, cost-sharing and coverage can vary. Some plans don’t cover services such as extractions and endodontics, which includes root canals. Most plans that cover these more extensive dental services require some combination of coinsurance, copayments and annual limits.
Even when information is fully available, mistakes are likely.
At 65, when most beneficiaries first enroll in Medicare, federal regulations guarantee that anyone can get Medigap coverage. During this initial sign-up, beneficiaries can’t be charged a higher premium based on their health.
Older Americans who enroll in a Medicare Advantage plan but then want to switch back to traditional Medicare after more than a year has passed lose that guarantee. This can effectively lock them out of enrolling in supplemental Medigap insurance, making the initial decision a one-way street.
For the initial sign-up, Medigap plans are “guaranteed issue,” meaning the plan must cover preexisting health conditions without a waiting period and must allow anyone to enroll, regardless of health. They also must be “community rated,” meaning that the cost of a plan can’t rise because of age or illness, although it can go up due to other factors such as inflation.
People who enroll in traditional Medicare and a supplemental Medigap plan at 65 can expect to continue paying community-rated premiums as long as they remain enrolled, regardless of what happens to their health.
In most states, however, people who switch from Medicare Advantage to traditional Medicare don’t have as many protections. Most state regulations permit plans to deny coverage, impose waiting periods or charge higher Medigap premiums based on their expected health costs. Only Connecticut, Maine, Massachusetts and New York guarantee that people can get Medigap plans after the initial sign-up period.
Deceptive advertising
Information about Medicare coverage and assistance choosing a plan is available but varies in quality and completeness. Older Americans are bombarded with ads for Medicare Advantage plans that they may not be eligible for and that include misleading statements about benefits.
A November 2022 report from the U.S. Senate Committee on Finance found deceptive and aggressive sales and marketing tactics, including mailed brochures that implied government endorsement, telemarketers who called up to 20 times a day, and salespeople who approached older adults in the grocery store to ask about their insurance coverage.
The Department of Health and Human Services tightened rules for 2024, requiring third-party marketers to include federal resources about Medicare, including the website and toll-free phone number, and limiting the number of contacts from marketers.
Although the government has the authority to review marketing materials, enforcement is partially dependent on whether complaints are filed. Complaints can be filed with the federal government’s Senior Medicare Patrol, a federally funded program that prevents and addresses unethical Medicare activities.
Nearly one-third of Medicare beneficiaries seek information from an insurance broker. Brokers sell health insurance plans from multiple companies. However, because they receive payment from plans in exchange for sales, and because they are unlikely to sell every option, a plan recommended by a broker may not meet a person’s needs.
Help is out there − but falls short
An alternative source of information is the federal government. It offers three sources of information to assist people with choosing one of these plans: 1-800-Medicare, medicare.gov and the State Health Insurance Assistance Program, also known as SHIP.
Telephone SHIP services are available nationally, but one of us and our colleagues have found that in-person SHIP services are not available in some areas. We tabulated areas by ZIP code in 27 states and found that although more than half of the locations had a SHIP site within the county, areas without a SHIP site included a larger proportion of people with low incomes.
Virtual services are an option that’s particularly useful in rural areas and for people with limited mobility or little access to transportation, but they require online access. Virtual and in-person services, where both a beneficiary and a counselor can look at the same computer screen, are especially useful for looking through complex coverage options.
As one SHIP coordinator noted, many people are not aware of all their coverage options. For instance, one beneficiary told a coordinator, “I’ve been on Medicaid and I’m aging out of Medicaid. And I don’t have a lot of money. And now I have to pay for my insurance?” As it turned out, the beneficiary was eligible for both Medicaid and Medicare because of their income, and so had to pay less than they thought.
The interviews made clear that many people are not aware that Medicare Advantage ads and insurance brokers may be biased. One counselor said, “There’s a lot of backing (beneficiaries) off the ledge, if you will, thanks to those TV commercials.”
Many SHIP staff counselors said they would benefit from additional training on coverage options, including for people who are eligible for both Medicare and Medicaid. The SHIP program relies heavily on volunteers, and there is often greater demand for services than the available volunteers can offer. Additional counselors would help meet needs for complex coverage decisions.
The key to making a good Medicare coverage decision is to use the help available and weigh your costs, access to health providers, current health and medication needs, and also consider how your health and medication needs might change as time goes on.
This article is part of an occasional series examining the U.S. Medicare system.
This story has been updated to remove a graphic that contained incorrect information about SHIP locations, and to correct the date of the open enrollment period.
Grace McCormack, Postdoctoral researcher of Health Policy and Economics, University of Southern California and Melissa Garrido, Research Professor, Health Law, Policy & Management, Boston University
This article is republished from The Conversation under a Creative Commons license.




 1. Younger Generations are More Likely to Report Mental Health Struggles, Worsening Mental Health
1. Younger Generations are More Likely to Report Mental Health Struggles, Worsening Mental Health










{kind=link}